
I didn’t craft that phrase, Florence Nightingale did in her 1860 book Notes on Nursing: What It Is and What It Is Not regarding unnecessary noise in nursing units. That’s right, 1860. This problem has been around for a while. Her judgment, “Unnecessary noise, then, is the most cruel absence of care which can be inflicted either on the sick or well.” wasn’t just a one-sentence comment. The entirety of chapter 4 is committed to the topic and simply titled “Noise.”
From one standpoint, all of the concerns about the ill effects of noise get summed up in a single number: your hospital’s score on the HCAHPS question “Patients who reported that the area around their room was “Always” quiet at night.” This patient experience question probably isn’t currently your lowest score but if your institution is like most, it was your lowest scoring question until the “Transition of Care” question was introduced in 2013. Expertise in design and planning can’t help you raise most of your HCAHPS scores but it can definitely help with this one.
What’s the real question?
One way to think about the problem is to identify the sources and then to develop strategies for each. Many studies have identified the harmful effects of noise (often associated with loss of sleep) and a few have quantified the perception of which noises are most noticeable – a perceptual combination of loudness, suddenness and frequency of occurrence. One interesting study had a simple summary of those results:
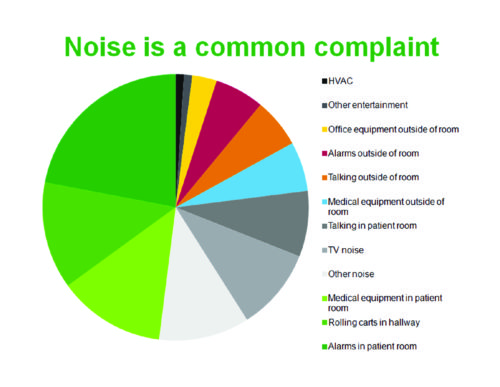
This study was carried out in acute level nursing units so those alarms and equipment in the patient room don’t represent the extremes of an ICU setting. The only item that can be directly attributed to the physical building itself is the 12th and last item on the list: HVAC noise. Everything else is hospital equipment or human activity.
Strategies for Improvement
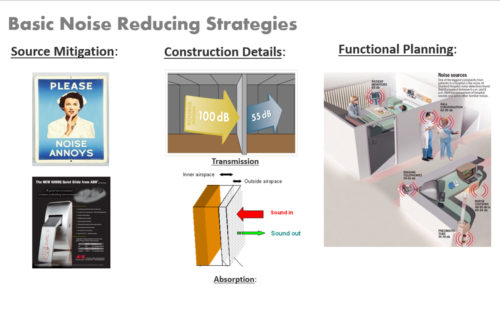
Noise reducing strategies fall into three categories: Source Mitigation, Construction Details (sound attenuation), and Functional Planning. Most of the aspects of the three interact, meaning that there isn’t a single or best answer to any given question.
When thinking of planning a new nursing unit, attention often quickly swings to the “soundproofing” of the construction. The issue is valid and needs thoughtful attention to its implementation, but the idea that the noise problem will be solved by designing to a minimum construction standard has a flaw – there’s little evidence that it is true. To test my intuition that “soundproofing” alone was not sufficient, I made a list of regional hospitals that have most of their beds in nursing units of roughly the same vintage, estimated the date of construction as best I could and then looked up their “Always Quiet” scores. The results support my experience and intuition. The average of the group is 62 which is within a point of the average state and national scores. If construction detailing alone would improve the score of any given hospital, one would expect scores to rise over time with the refinement of minimum sound attenuation standards in the Federal Guidelines. This graphic doesn’t seem to support the hypothesis of gradual improvement over time as building design standards were improved.
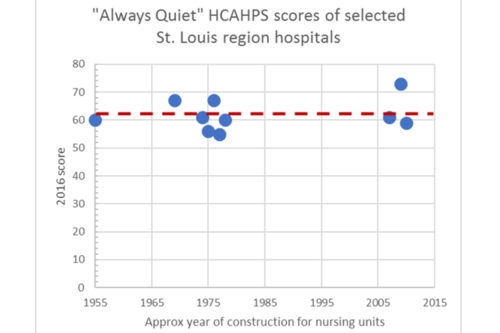
My conclusion: meeting the construction “soundproofing” guidelines is necessary but not sufficient.
Extending the Benefit of Better Design
So, if construction detailing isn’t the complete answer, what is? Figure 2 also identifies source mitigation and functional planning as remaining parts of the strategy and if you look again at Figure 1, the most noticeable sources are identified. The most effective strategy looks at these two approaches in combination because they have overlaps.
In 2016, Jeff Johnston of Mercy and John Reeve of Christner presented the results of a post-occupancy evaluation (POE) of the Heart Hospital addition to the Mercy St. Louis campus. One focus of the POE study was nursing unit acoustics and was able to characterize the patient’s acoustic experience by measuring sound levels utilizing a “cloud” of sensors that provided a multi-point, 24-hour, continuous data set. (You can review the full slide deck of their presentation here: link) The outcomes are convincing and provide a clear indication about the real benefits of insightful planning.
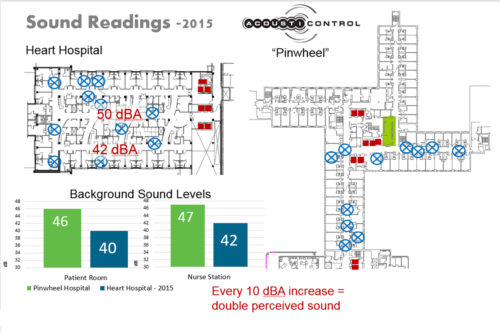
Design of the Heart Hospital floor plate employed several strategies to both mitigate sources directly and to move sources away from the inpatient rooms. The older “pinwheel” plan that served as the comparison was well-built but was very much a product of the times in which the phrase “planning efficiency” translated into minimum dimensions, minimum space and minimum circulation. As it turns out, all these “minimums” came at a price that has been paid by patients ever since – trying to recuperate in a noisy environment. The newer Heart Hospital plan utilized several planning ideas to improve patient experience: distributed nursing stations, enclosure/separation of noise generators and an innovative “third” corridor that was the designated route for most of the service traffic.
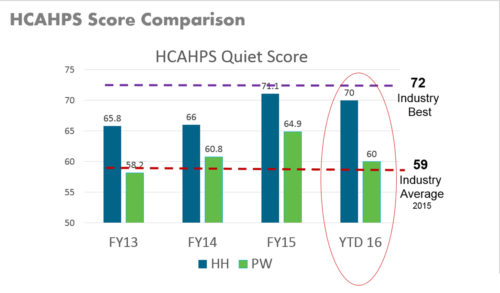
Does a 6 dBA difference in room background sound translate into a better HCAHPS score? This empirical evidence says ”yes.” When Mercy compiled HCAHPS scores separately for the two nursing units, the difference has been consistently about 6 points, placing the performance of the Heart Hospital (noted as “HH” in the legend) nursing units very close to the best of all nationally reported performance!
In terms of construction detailing, the soundproofing details of this new unit design were not different from those we use on most of the nursing units we design and certainly met the minimum “soundproofing” standards in effect at the time. I am convinced that the significant improvements in the Heart Hospital scores has its foundation not in the construction details but in the many thoughtful choices recommended by Christner planners.
(Neonatal patients do not fill out experience surveys but Christner’s Shanna Wiechel has nonetheless presented on the improvement of acoustics in the neonatal intensive care unit. You can see an excerpt of the presentation she made on this and related topics with SSM’s Karen Rewerts here: link)
A couple of closing thoughts: take another look at the perceived noise sources in Figure 1 and note how many relate to the equipment you buy. Have you challenged Clinical Engineering and Purchasing to set clear performance criteria for quiet operation? I know from personal observation that the ubiquitous, grey plastic trash barrel on casters can make such a rumble when pushed down the corridor that it made one struggling, elderly, disoriented patient believe that the building was collapsing. It certainly wasn’t good for her heart rate and maybe even represented “a cruel absence of care.”

